Stroke Center & Department of Neurology, The First Affiliated Hospital of USTC, Division of Life Sciences and Medicine, University of Science and Technology of China, Hefei 230036, China
Fengling Qu is currently a master’s student in the Department of Life Sciences and Medicine, University of Science and Technology of China, under the supervision of Prof. Xinfeng Liu. Her research mainly focuses on relapse and progression of demyelinating diseases
Chunrong Tao is currently an Attending Physician in the Department of Neurology, the First Affiliated Hospital of USTC. He received his Ph.D. degree in Neurology from the University of Science and Technology of China in 2019. His research mainly focuses on epidemiology
Wei Hu is currently a Chief Physician in the Department of Neurology, the First Affiliated Hospital of USTC. He received his Ph.D. degree in Neurology from Anhui Medical University in 2017. His research mainly focuses on the pathogenesis of cerebral collateral circulation and ischemic stroke
Xinfeng Liu is currently a Professor in the Department of Life Sciences and Medicine, University of Science and Technology of China. He received his Ph.D. degree in Neurology from the University of Lausanne, Switzerland, in 2001. His research mainly focuses on interventional diagnosis and treatment of cerebrovascular diseases
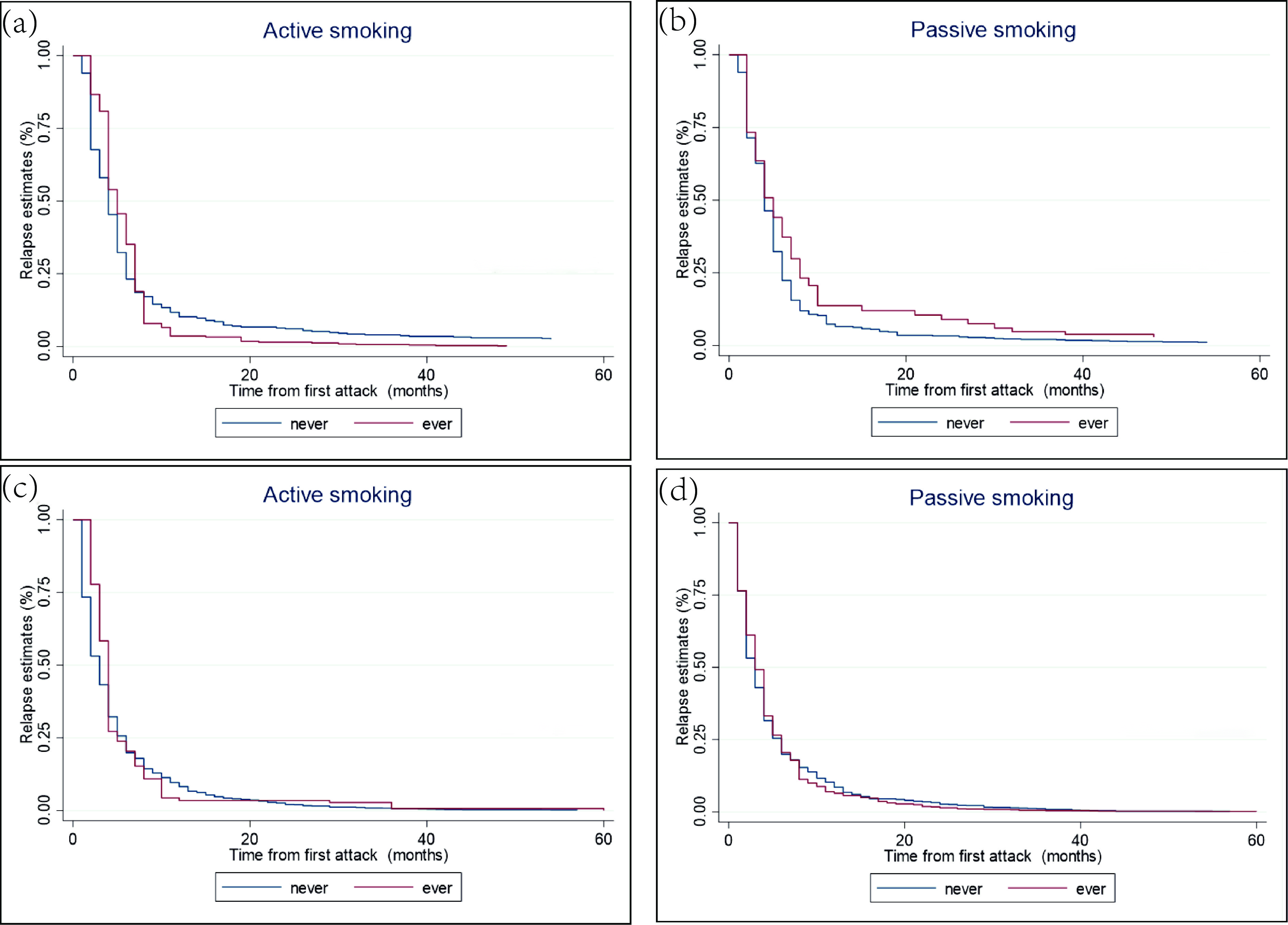
Objective: Active and passive smoking are common environmental risk factors, but there is no definite conclusion about their effects on relapse and disability progression in multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD). Methods: This was a retrospective cohort study. Patients were included from four centers. Demographic and clinical data were extracted from the clinical database, while data involving environmental exposures during daily life, relapse, and disability progression were obtained through telephone follow-up interviews. Determinants of relapse were assessed by Cox proportional models, and disability progression was assessed by linear regression. Kaplan‒Meier survival was used to estimate relapse within five years after the first attack. Results: A total of 130 MS patients and 318 NMOSD patients were included in this study, and females accounted for 60% and 79.6%, respectively. MS patients with an active smoking history had a higher risk of relapse, for which the association became borderline significant after accounting for covariates (aHR=1.52, 95% CI=1.00, 2.31; p=0.052). The relapse risk between ever-smokers who smoked more than 10 cigarettes per day and smokers who smoked less than 10 cigarettes per day was not significantly different (aHR=0.96, 95% CI=0.63, 1.47; p=0.859). However, exposure to passive smoking was associated with a reduced risk of MS relapse (aHR=0.75, 95% CI=0.56, 1.00; p=0.044) compared with never-exposed patients. No associations were observed between active smoking/passive smoking and the risk of NMOSD relapse, but patients with a history of smoking were associated with a lower annual progression rate by Expanded Disability Status Scale (EDSS) (aβ=−0.20, 95% CI=−0.38, −0.01; p=0.036) and Multiple Sclerosis Severity Score (MSSS) (aβ=−0.23, 95% CI=−0.44, −0.03; p=0.028). Conclusion: Our research shows that active smoking increases the relapse risk of MS and has a negative impact on disability progression; thus, smoking cessation should be encouraged.
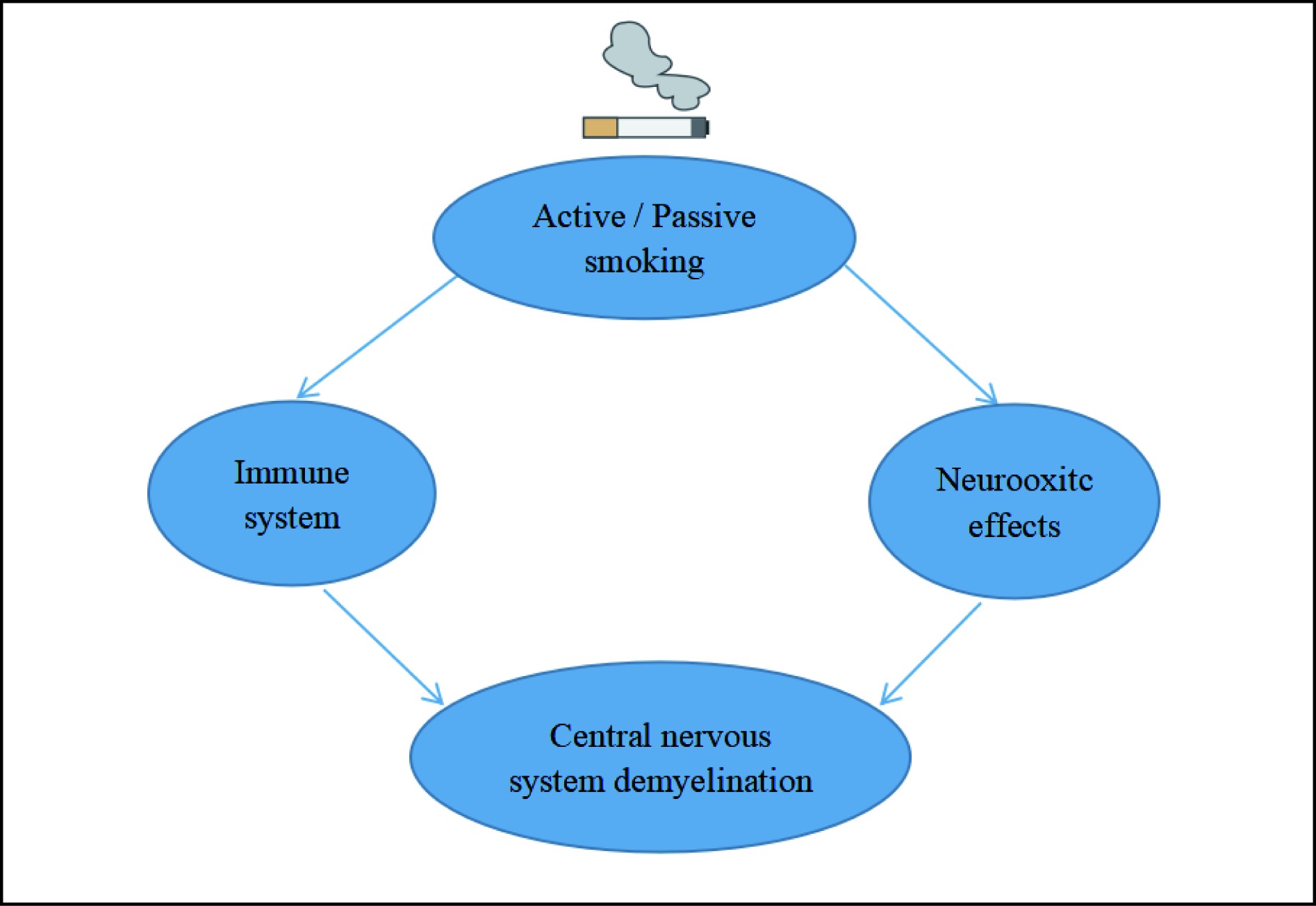
Graphical Abstract
The mechanism of cigarette smoke affecting demyelinating diseases.
Abstract
Objective: Active and passive smoking are common environmental risk factors, but there is no definite conclusion about their effects on relapse and disability progression in multiple sclerosis (MS) and neuromyelitis optica spectrum disorder (NMOSD). Methods: This was a retrospective cohort study. Patients were included from four centers. Demographic and clinical data were extracted from the clinical database, while data involving environmental exposures during daily life, relapse, and disability progression were obtained through telephone follow-up interviews. Determinants of relapse were assessed by Cox proportional models, and disability progression was assessed by linear regression. Kaplan‒Meier survival was used to estimate relapse within five years after the first attack. Results: A total of 130 MS patients and 318 NMOSD patients were included in this study, and females accounted for 60% and 79.6%, respectively. MS patients with an active smoking history had a higher risk of relapse, for which the association became borderline significant after accounting for covariates (aHR=1.52, 95% CI=1.00, 2.31; p=0.052). The relapse risk between ever-smokers who smoked more than 10 cigarettes per day and smokers who smoked less than 10 cigarettes per day was not significantly different (aHR=0.96, 95% CI=0.63, 1.47; p=0.859). However, exposure to passive smoking was associated with a reduced risk of MS relapse (aHR=0.75, 95% CI=0.56, 1.00; p=0.044) compared with never-exposed patients. No associations were observed between active smoking/passive smoking and the risk of NMOSD relapse, but patients with a history of smoking were associated with a lower annual progression rate by Expanded Disability Status Scale (EDSS) (aβ=−0.20, 95% CI=−0.38, −0.01; p=0.036) and Multiple Sclerosis Severity Score (MSSS) (aβ=−0.23, 95% CI=−0.44, −0.03; p=0.028). Conclusion: Our research shows that active smoking increases the relapse risk of MS and has a negative impact on disability progression; thus, smoking cessation should be encouraged.
Public Summary
We evaluated the impact of passive smoking on multiple sclerosis (MS) relapse and disability progression.
Compared to never-smokers, patients with MS who actively smoke have a significantly increased risk of relapse.
In MS, compared to never-smokers, active smokers experience accelerated disability progression.
China has firmly set the goal of peak carbon emissions before 2030 and full carbon neutrality before 2060[1-3]. Against this background, the new energy vehicle (NEV) industry presents a new space for rapid growth. To promote the development of the NEV industry, China has successively issued a series of subsidies since 2009[4, 5]. In 2013, as the development of the NEV industry entered a new stage, China began to implement its program of retrogressive subsidies (PRS)1. The purpose of this policy is to reduce the impact of government intervention in the NEV industry by reducing the amount of subsidies year by year and to give full play to the decisive role of the market in resource allocation. Prior studies have shown that subsidies have promoted the development of China’s NEV industry[6, 7].
The COVID-19 pandemic, a major public emergency, has a significantly negative impact on human society. To cope with the negative influence of the COVID-19 pandemic on China’s NEV enterprises, the Chinese government issued the latest PRS on April 23, 2020, stating that China has decided to extend it until 2022, after which it may be completely cancelled2. Although previous scholars have conducted in-depth studies on the reaction of NEV enterprises’ stakeholders to the subsidy policy and the resulting change in enterprises’ performance, most of them tend to focus only on the reaction of corporate consumers to the subsidy policy and the resulting change in enterprises’ financial or innovation performance[8, 9]. As a result, they have ignored the reaction of corporate investors to the subsidy policy and the resulting change in the corporate market value. On the other hand, prior scholars have always tended to investigate the reaction of stakeholders to subsidy policies in the context of corporate daily operations[10-12]. However, few scholars have paid attention to it in the context of major public emergencies, such as COVID-19 pandemic. Based on this, this research aims to explore the reaction mechanism of NEV enterprise investors to the PRS in the context of COVID-19 pandemic.
Overall, based on the event study method, this study empirically tested the reaction mechanism of investors of NEV enterprises to China’s PRS in the context of COVID-19 pandemic and discussed the differences in investors’ reactions under different enterprise attributes (i.e., whether listed on the Shanghai Stock Exchange, whether located in a first-tier city, whether belonging to state-owned enterprises, and whether belonging to the upstream NEV industry).
The rest of the paper is organized as follows. Section 2 introduces the theoretical background and develops our hypotheses. Section 3 introduces the research design, and Section 4 analyzes the empirical results. The last section is the conclusions.
2.
Theoretical background and hypothesis development
2.1
The reaction of NEV enterprise investors to the PRS in the context of COVID-19 pandemic
Prospect theory was first proposed in 1979, which points out that people are different in their sensitivity to loss and gain, and the pain in the face of loss is much greater than the pleasure in the face of gain[13-16]. Therefore, when choosing between a certain profit and a risky gamble, people often choose a certain profit to avoid the risk of loss[17-19]. From an investor’s point of view, investors are generally reluctant to take risks[20]. For different investment projects with the same rate of return, investors will always choose the investment projects with the lowest risk[21, 22]. Based on this, investors’ perception of the future risks and benefits of the NEV industry will affect their behavioral feedback to NEV enterprises, which in turn affects the market value of NEV enterprises.
The NEV subsidy policy is crucial to the survival and development of the NEV industry in China[23, 24]. During the past ten years, the subsidy policy for NEVs has greatly stimulated consumers’ enthusiasm for purchasing NEVs and investors’ desire to invest in the enterprises that produce them, which has effectively promoted the development of the NEV industry in China[25, 26]. However, the sudden outbreak of COVID-19 in 2019 disrupted the orderly development of China’s NEV industry. To cope with its negative influence on China’s NEV enterprises, the Chinese government issued the latest PRS on April 23, 2020. However, due to information asymmetry, stakeholders may misunderstand this subsidy policy; that is, they may hold that the government will not have other subsidy policies after the implementation of the PRS. Therefore, investors may be concerned about the future development of NEV enterprises. In this case, based on the perspective of prospect theory, investors may be more inclined to place their funds in lower-risk industries. Based on the above logic, we assume the following hypothesis:
Hypothesis 1. The reaction of NEV enterprise investors to the PRS in the context of COVID-19 pandemic is likely to be negative.
2.2
The heterogeneous reaction of NEV enterprise investors: Shanghai vs. Shenzhen Stock Exchanges
Generally, the Shanghai Stock Exchange is dominated by large enterprises with stable performance, while the Shenzhen Stock Exchange is dominated by small- and medium-sized enterprises that are in their developmental stages[27, 28]. Therefore, on the whole, compared with enterprises listed on the Shenzhen Stock Exchange, enterprises listed on the Shanghai Stock Exchange are generally more equipped to manage uncertainties and risks. In this case, investors of NEV enterprises listed on the Shanghai Stock Exchange (vs. the Shenzhen Stock Exchange) should have a lower risk perception when facing the PRS in the context of COVID-19 pandemic. Based on the above logic, we assume the following hypothesis:
Hypothesis 2. The negative reaction of investors is weaker when NEV enterprises are listed on the Shanghai Stock Exchange (vs. the Shenzhen Stock Exchange).
2.3
The heterogeneous reaction of NEV enterprise investors: state-owned vs. nonstate-owned enterprises
State-owned enterprises, which act in an agency capacity on behalf of the government in the market economy[29, 30], are granted sufficient resources[31, 32], such as policy and industry information[33], subsidies[34] and tax breaks[35], by the state. These political resources can help such enterprises effectively cope with risks and unforeseen challenges[36–38]. Therefore, even after the issuance of the PRS in response to COVID-19 pandemic, state-owned enterprises still enjoy more resources than nonstate-owned enterprises in the postsubsidy era. As such, investors in nonstate-owned NEV enterprises should have a higher risk perception given the anticipated effects of the PRS. Based on the above logic, we assume the following hypothesis:
Hypothesis 3. The negative reaction of investors is stronger when NEV enterprises belong to nonstate-owned enterprises (vs. state-owned enterprises).
2.4
The heterogeneous reaction of NEV enterprise investors: first-tier cities vs. nonfirst-tier cities
Generally, first-tier cities have a higher level of economic development than nonfirst-tier cities. Therefore, the local governments in first-tier cities usually have a stronger ability to support local enterprises in the postsubsidy era. In addition, enterprises that can survive in first-tier cities usually have more resistance to uncertainties and risks than those in nonfirst-tier cities. In this case, investors in NEV enterprises in first-tier cities (vs. nonfirst-tier cities) should have a lower risk perception in response to the PRS in the context of COVID-19 pandemic. Based on the above logic, we assume the following hypothesis:
Hypothesis 4. The negative reaction of investors is weaker when NEV enterprises are located in first-tier cities (vs. nonfirst-tier cities).
2.5
The heterogeneous reaction of NEV enterprise investors in the supply chain
At present, the number of upstream enterprises is much higher than that of midstream and downstream enterprises in China’s NEV industry, which means that upstream enterprises will face greater competitive pressure when dealing with the uncertainties associated with future industry development. In other words, investors in upstream enterprises (vs. midstream and downstream enterprises) are more risk-aware when facing uncertainties. In this case, investors in upstream enterprises (vs. midstream and downstream enterprises) should have a higher risk perception in response to the PRS in the context of COVID-19 pandemic. Based on the above logic, we assume the following hypothesis:
Hypothesis 5. The negative reaction of investors is stronger for upstream (vs. midstream and downstream) NEV enterprises.
3.
Research design
3.1
Sample selection and data source
A total of 171 automobile enterprises listed on the Shenzhen and Shanghai Stock Exchanges were selected as samples in this study. Specifically, the sample source is Choice3, which is among the top financial databases in China. Based on the industry classification of listed enterprises by Choice, we obtained a sample of 209 listed enterprises whose main line of business is in the automobile industry. Considering that this study focuses on the PRS issued on April 23, 2020, we excluded 31 samples with market dates after April 23, 2020. Additionally, to prevent confounding events that fall within seven days of the issuance of the PRS and to avoid using an insufficient return prediction period, we also removed 7 unqualified samples[39, 40]. After accounting for these considerations, we obtained a sample of 171 listed auto enterprises, of which 109 are considered NEV enterprises and 62 are considered nonnew energy vehicle (NNEV) enterprises based on the classification set forth by Choice.
Cumulative abnormal return (CAR) is the explanatory variable we use to probe the effect of the PRS on corporate market value. Following prior studies, CAR related to the critical event is calculated within a 3-day time window (i.e., −1,0,and+1 days) [41]. Concretely:
Abnormal return (AR) refers to the unexpected percentage difference between the expected normal and actual returns. The market model is used to calculate the normal return, AR and CAR[40], namely:
Rit=Ii+SiRmt+ETit,
where Rit is the normal return of security i on day t, Ii is the intercept, Si is the systematic risk related to security i, Rmt is the return on the market portfolio of stocks on day t, and ETit is the error term of security i on day t.
Next, AR is calculated as:
ARit=Rit−(Xi+ZiRmt),
where ARit is the AR of security i on day t and Xi and Zi belong to the ordinary least squares (OLS) parameter estimates of security i. CAR for the 3-day time window for each security i is thus calculated as
CAR(−1,0,+1)=n=(−1,0,+1)∑t=nARit.
The expected normal returns are estimated using a trailing period of 128 to 8 trading days before the critical event[40]. We regard the PRS issued on April 23, 2020, as the critical event. Since the policy promulgation time (17:08) is the closing time of the stock market on that day (13:00–15:00), we choose April 24, 2020, as the event date. The daily market return volatility is calculated using the equal weight average of the Shanghai Stock Exchange Composite Index and the Shenzhen Stock Exchange Component Index[40-42]. All data were collected from the CSMAR4.
3.2.2
Explanatory variable
Whether it is an NEV enterprise: If the firm is classified as a new energy concept by Choice, it is considered to be an NEV enterprise and given the value of “1”; otherwise, it is given the value of “0”.
Listed on the Shanghai Stock Exchange: If the firm is listed on the Shanghai Stock Exchange, it is given the value of “1”; otherwise, it is given the value of “0”.
Whether it is a state-owned enterprise: If the firm is ultimately controlled by the State-Owned Assets Committee of China, it is given the value of “1”; otherwise, it is given the value of “0”.
Is it located in the first-tier city: If the firm was headquartered in a first-tier city (i.e., Beijing, Shanghai, Guangzhou and Shenzhen) in 2020, it is given the value of “1”; otherwise, it is given the value of “0”.
Supply chain position: If the firm is mainly engaged in supplying raw materials and accessories/automobile manufacturing/vehicle sales, it is considered to be in the upstream/midstream/downstream of the supply chain and given the value of “1”; otherwise, it is given the value of “0”.
3.2.3
Descriptive statistics
Tables 1 and 2 show the statistical data of the variables.
3.2.4
Kolmogorov–Smirnov (KS) test and Wilcoxon signed-rank test
To explore the effect of the PRS on the market value of NEV enterprises, we decided to follow Lo et al.[43] by applying the methods of an independent sample t-test or a Wilcoxon signed-rank test. Through the KS test, we found that all explained variables did not conform to the normal distribution (see Table 3); thus, the Wilcoxon signed-rank test was adopted (compared to the default median “0”).
It can be seen from Table 4 that the negative reaction of NEV enterprise investors is significant (Day−1to1,z=−3.048, p=0.002), while the negative reaction of NNEV enterprise investors is not significant (Day −1 to 1, z=0.007, p=0.994). Hypothesis 1 is thus proven. Additionally, Day −1 is not significant, thus indicating that no information is leaked before the event.
Table
4.
Wilcoxon signed-rank test between NEV and NNEV enterprises.
We further analyze charts of the stock market to identify the reaction of investors (see Fig. 1). Fig. 1 shows that the AAR is significantly negative from the first day (Day 0) and reaches the negative pole on the third day (Day 2). This reveals a coupling relationship between the dissemination period of policy information and the negative reaction of investors.
Figure
1.
NEV enterprise investors’ reaction to the PRS.
Table 5 reveals the difference in the reaction of investors of NEV enterprises listed on the Shanghai and Shenzhen Stock Exchanges. Table 5 shows that the market value of NEV enterprises listed on the Shenzhen Stock Exchange suffers a greater negative impact (Day −1 to 1, z=−4.022, p=0.000). Hypothesis 2 is therefore tested. The results show that investors have more confidence in NEV enterprises on the Shanghai Stock Exchange (vs. the Shenzhen Stock Exchange) in the postsubsidy era.
Table
5.
Wilcoxon signed-rank test between the Shanghai and Shenzhen Stock Exchanges.
Table 6 shows the difference in the reaction of investors of state-owned and nonstate-owned firms. From Table 6, it can be seen that the market value of nonstate-owned enterprises suffers a greater negative impact (Day −1 to 1, z=−3.115, p=0.002). Hypothesis 3 is thus proven. Our results echo those of Wang et al.[8] and support our view that state-owned NEV enterprises have more political resources to ensure their survival and development, and their investors will thus have higher confidence in their development prospects in the postsubsidy era.
Table
6.
Wilcoxon signed-rank test between state-owned and nonstate-owned firms.
Table 7 shows the difference in the reaction of investors of NEV enterprises in different geographical locations. Table 7 shows that the market value of NEV enterprises located in first-tier cities suffers a less negative impact (Day −1 to 1, z=−1.704, p=0.088). Hypothesis 4 is thus proven. Our results confirm our view that investors will have more confidence in NEV enterprises located in first-tier cities (vs. nonfirst-tier cities) in the postsubsidy era.
Table
7.
Wilcoxon signed-rank test between first-tier cities and nonfirst-tier cities.
Table 8 shows the difference in the reaction of investors of NEV enterprises with different supply chain locations. It can be seen from Table 8 that the market value of NEV enterprises located in the upstream market segment suffers a greater negative impact (Day −1 to 1, z=−2.792, p=0.005). Hypothesis 5 is thus proven. Our results confirm our view that investors may have less confidence in upstream (vs. midstream and downstream) NEV enterprises in the postsubsidy era.
Table
8.
Wilcoxon signed-rank test in the supply chain.
First, the results of Day 0, Day 1, and Day 0 to 1 in Tables 4 to 8 are consistent with Day −1 to 1, thus indicating the robustness of our results. Second, to verify the validity of the Wilcoxon signed-rank test, the binomial sign test was selected as an alternative method (see Tables S1−S5 in Supporting Information). Our key results remain unchanged. Finally, we regard the new first-tier cities determined in 2020 as first-tier cities and empirically retest the first-tier cities variable. The results remain robust (see Tables S6 and S7 in Supporting Information).
5.
Conclusions
COVID-19 pandemic has a serious negative impact on China’s economy, especially in the NEV industry, which is in its early developmental stages. To address the negative impact of COVID-19 pandemic on China’s NEV industry, the Chinese government issued the latest PRS on April 23, 2020. To explore the reaction mechanism of NEV enterprise investors to the PRS in the context of COVID-19 pandemic, 171 Chinese listed auto enterprises were selected as samples. Based on the event study method, this study discussed the differences in investors’ reactions under different enterprise attributes (i.e., whether listed on the Shanghai Stock Exchange, whether located in a first-tier city, whether belonging to state-owned enterprises, and whether belonging to the upstream NEV enterprises. Overall, we obtained five results. First, due to information asymmetry, the reaction of NEV enterprise investors to the PRS in the context of COVID-19 pandemic is negative. Second, the negative reaction of investors is weaker when NEV enterprises are listed on the Shanghai Stock Exchange (vs. the Shenzhen Stock Exchange). Third, the negative reaction of investors is stronger when NEV enterprises belong to nonstate-owned enterprises (vs. state-owned enterprises). Fourth, the negative reaction of investors is weaker when NEV enterprises are located in first-tier cities (vs. nonfirst-tier cities). Finally, the negative reaction of investors is stronger for upstream (vs. midstream and downstream) NEV enterprises. Overall, the results of this study provide empirical evidence for the effectiveness of risk aversion in prospect theory in practice and enrich the application scenario of prospect theory.
This study’s contribution to the literature is threefold. First, our study provides empirical evidence for analyzing the reaction of NEV enterprise investors to the government subsidy policy, which enriches the literature focusing on the reaction of stakeholders to the government subsidy policy. Second, this study analyzes the reaction of NEV enterprise investors to the PRS in the context of COVID-19 pandemic from multiple perspectives, thus providing practical insight for NEV enterprises to make decisions on stakeholder management strategies in the context of major public emergencies. Finally, by comparing and analyzing the degree of change in the market value of NEV enterprises with different attributes when the PRS is issued, our study provides practical recommendations on how to formulate government policy response strategies according to the unique needs of each situation.
Our study also makes several practical recommendations for NEV enterprises and their investors. First, when the state announces subsidy policies similar to PRS, enterprises should communicate information with external investors in a timely manner to prevent losses caused by stakeholders’ misunderstanding, especially in the context of major public emergencies, such as COVID-19 pandemic. Second, NEV enterprises should convey reliable signals to investors in the daily operation process to prevent them from suffering market value loss in the context of information asymmetry, especially for nonstate-owned enterprises, enterprises in the Shenzhen Stock Exchange and nonfirst-tier cities, as well as upstream enterprises with greater pressure of competition. Finally, investors of NEV enterprises should believe in the scientific nature and effectiveness of national policies to avoid causing their own losses due to misunderstanding.
Our research also presents several limitations. On the one hand, this study only focuses on NEV enterprises in the automobile industry. There are other firms in other industries related to NEV, which can be included in the sample for further exploration in future research. On the other hand, this study only focuses on the key subsidy policy made by the government in response to COVID-19 pandemic. As the situation of the epidemic changes, the government may introduce other follow-up policies. Therefore, future research can continue to explore the reaction mechanism of NEV enterprise investors to other policies on the basis of this study.
Acknowledgements
This work was supported by the National Natural Science Foundation of China (U20A20357) and Program for Innovative Research Team of the First Affiliated Hospital of USTC.
Conflict of interest
The authors declared that they had no conflict of interest.
We evaluated the impact of passive smoking on multiple sclerosis (MS) relapse and disability progression.
Compared to never-smokers, patients with MS who actively smoke have a significantly increased risk of relapse.
In MS, compared to never-smokers, active smokers experience accelerated disability progression.
Höftberger R, Lassmann H. Inflammatory demyelinating diseases of the central nervous system. Handb. Clin. Neurol.,2017, 145: 263–283. DOI: 10.1016/B978-0-12-802395-2.00019-5
[2]
Lennon V A, Wingerchuk D M, Kryzer T J, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet,2004, 364 (9451): 2106–2112. DOI: 10.1016/S0140-6736(04)17551-X
[3]
Tian D C, Zhang C Y, Yuan M, et al. Incidence of multiple sclerosis in China: A nationwide hospital-based study. Lancet Reg. Health West. Pac.,2020, 1: 100010. DOI: 10.1016/j.lanwpc.2020.100010
[4]
Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: A review. JAMA Neurol.,2020, 77 (2): 245–253. DOI: 10.1001/jamaneurol.2019.4271
[5]
Messina S, Mariano R, Geraldes R, et al. The influence of smoking on the pattern of disability and relapse risk in AQP4-positive Neuromyelitis Optica Spectrum Disorder, MOG-Ab Disease and Multiple Sclerosis. Mult. Scler. Relat. Disord.,2021, 49: 102773. DOI: 10.1016/j.msard.2021.102773
[6]
Lavery A M, Collins B N, Waldman A T, et al. The contribution of secondhand tobacco smoke exposure to pediatric multiple sclerosis risk. Mult. Scler.,2019, 25 (4): 515–522. DOI: 10.1177/1352458518757089
[7]
Pittas F, Ponsonby A L, van der Mei I A F, et al. Smoking is associated with progressive disease course and increased progression in clinical disability in a prospective cohort of people with multiple sclerosis. J. Neurol.,2009, 256 (4): 577–585. DOI: 10.1007/s00415-009-0120-2
[8]
Petersen E R, Oturai A B, Koch-Henriksen N, et al. Smoking affects the interferon beta treatment response in multiple sclerosis. Neurology,2018, 90 (7): e593–e600. DOI: 10.1212/WNL.0000000000004949
[9]
Munger K L, Fitzgerald K C, Freedman M S, et al. No association of multiple sclerosis activity and progression with EBV or tobacco use in BENEFIT. Neurology,2015, 85 (19): 1694–1701. DOI: 10.1212/WNL.0000000000002099
[10]
Weiland T J, Hadgkiss E J, Jelinek G A, et al. The association of alcohol consumption and smoking with quality of life, disability and disease activity in an international sample of people with multiple sclerosis. J. Neurol. Sci.,2014, 336: 211–219. DOI: 10.1016/j.jns.2013.10.046
[11]
Kvistad S, Myhr K M, Holmøy T, et al. No association of tobacco use and disease activity in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm.,2016, 3 (4): e260. DOI: 10.1212/NXI.0000000000000260
[12]
Briggs F B S, Yu J C, Davis M F, et al. Multiple sclerosis risk factors contribute to onset heterogeneity. Mult. Scler. Relat. Disord.,2019, 28: 11–16. DOI: 10.1016/j.msard.2018.12.007
[13]
Petersen E R, Søndergaard H B, Laursen J H, et al. Smoking is associated with increased disease activity during natalizumab treatment in multiple sclerosis. Mult. Scler.,2019, 25 (9): 1298–1305. DOI: 10.1177/1352458518791753
[14]
Polman C H, Reingold S C, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol.,2011, 69 (2): 292–302. DOI: 10.1002/ana.22366
[15]
Thompson A J, Banwell B L, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol.,2018, 17 (2): 162–173. DOI: 10.1016/S1474-4422(17)30470-2
[16]
Wingerchuk D M, Banwell B, Bennett J L, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology,2015, 85 (2): 177–189. DOI: 10.1212/WNL.0000000000001729
[17]
Hedström A K, Olsson T, Alfredsson L. Smoking is a major preventable risk factor for multiple sclerosis. Mult. Scler.,2016, 22 (8): 1021–1026. DOI: 10.1177/1352458515609794
[18]
Kurtzke J F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology,1983, 33 (11): 1444–1452. DOI: 10.1212/WNL.33.11.1444
[19]
Roxburgh R H S R, Seaman S R, Masterman T, et al. Multiple Sclerosis Severity Score: Using disability and disease duration to rate disease severity. Neurology,2005, 64 (7): 1144–1151. DOI: 10.1212/01.WNL.0000156155.19270.F8
[20]
Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology,2015, 44 (4): 199–214. DOI: 10.1159/000382130
[21]
Tettey P, Simpson S Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult. Scler.,2014, 20 (13): 1737–1744. DOI: 10.1177/1352458514533162
[22]
Manouchehrinia A, Tench C R, Maxted J, et al. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain,2013, 136: 2298–2304. DOI: 10.1093/brain/awt139
[23]
Ivashynka A, Copetti M, Naldi P, et al. The impact of lifetime alcohol and cigarette smoking loads on multiple sclerosis severity. Front. Neurol.,2019, 10: 866. DOI: 10.3389/fneur.2019.00866
[24]
Paz-Ballesteros W C, Monterrubio-Flores E A, de Jesús Flores-Rivera J, et al. Cigarette smoking, alcohol consumption and overweight in multiple sclerosis: disability progression. Arch. Med. Res.,2017, 48 (1): 113–120. DOI: 10.1016/j.arcmed.2017.03.002
[25]
D'hooghe M B, Haentjens P, Nagels G, et al. Alcohol, coffee, fish, smoking and disease progression in multiple sclerosis. Eur. J. Neurol.,2012, 19 (4): 616–624. DOI: 10.1111/j.1468-1331.2011.03596.x
[26]
Kinga M, Balasa R. Effect of serum 25(OH) D level, cigarette smoking and oral contraceptive use on clinical course of relapsing-remitting multiple sclerosis in a group of female patients. Romanian Journal of Neurology,2015, 14 (4): 214–218. DOI: 10.37897/RJN.2015.4.5
[27]
Al Wutayd O, Mohamed A G, Saeedi J, et al. Environmental exposures and the risk of multiple sclerosis in Saudi Arabia. BMC Neurol.,2018, 18 (1): 86. DOI: 10.1186/s12883-018-1090-8
[28]
Tao C, Simpson S Jr, Taylor B V, et al. Onset symptoms, tobacco smoking, and progressive-onset phenotype are associated with a delayed onset of multiple sclerosis, and marijuana use with an earlier onset. Front. Neurol.,2018, 9: 418. DOI: 10.3389/fneur.2018.00418
[29]
McDowell T Y, Amr S, Culpepper W J, et al. Sun exposure, vitamin D and age at disease onset in relapsing multiple sclerosis. Neuroepidemiology,2011, 36 (1): 39–45. DOI: 10.1159/000322512
[30]
Hedström A K, Hillert J, Olsson T, et al. Smoking and multiple sclerosis susceptibility. Eur. J. Epidemiol.,2013, 28 (11): 867–874. DOI: 10.1007/s10654-013-9853-4
[31]
Hedstrom A K, Baarnhielm M, Olsson T, et al. Tobacco smoking, but not Swedish snuff use, increases the risk of multiple sclerosis. Neurology,2009, 73 (9): 696–701. DOI: 10.1212/WNL.0b013e3181b59c40
[32]
Alrouji M, Manouchehrinia A, Gran B, et al. Effects of cigarette smoke on immunity, neuroinflammation and multiple sclerosis. J. Neuroimmunol.,2019, 329: 24–34. DOI: 10.1016/j.jneuroim.2018.10.004
[33]
Jin H J, Li H T, Sui H X, et al. Nicotine stimulated bone marrow-derived dendritic cells could augment HBV specific CTL priming by activating PI3K-Akt pathway. Immunol. Lett.,2012, 146: 40–49. DOI: 10.1016/j.imlet.2012.02.015
[34]
Gao Z, Nissen J C, Ji K, et al. The experimental autoimmune encephalomyelitis disease course is modulated by nicotine and other cigarette smoke components. PLoS One,2014, 9 (9): e107979. DOI: 10.1371/journal.pone.0107979
[35]
de Jonge W J, Ulloa L. The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br. J. Pharmacol.,2007, 151 (7): 915–929. DOI: 10.1038/sj.bjp.0707264
[36]
Tracey K J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Invest.,2007, 117 (2): 289–296. DOI: 10.1172/JCI30555
[37]
Filippini P, Cesario A, Fini M, et al. The Yin and Yang of non-neuronal α7-nicotinic receptors in inflammation and autoimmunity. Curr. Drug Targets,2012, 13 (5): 644–655. DOI: 10.2174/138945012800399008
Figure
1.
Kaplan‒Meier analysis of (a, b) time to relapse in the MS cohort and (c, d) time to relapse in the NMOSD cohort.
References
[1]
Höftberger R, Lassmann H. Inflammatory demyelinating diseases of the central nervous system. Handb. Clin. Neurol.,2017, 145: 263–283. DOI: 10.1016/B978-0-12-802395-2.00019-5
[2]
Lennon V A, Wingerchuk D M, Kryzer T J, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet,2004, 364 (9451): 2106–2112. DOI: 10.1016/S0140-6736(04)17551-X
[3]
Tian D C, Zhang C Y, Yuan M, et al. Incidence of multiple sclerosis in China: A nationwide hospital-based study. Lancet Reg. Health West. Pac.,2020, 1: 100010. DOI: 10.1016/j.lanwpc.2020.100010
[4]
Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: A review. JAMA Neurol.,2020, 77 (2): 245–253. DOI: 10.1001/jamaneurol.2019.4271
[5]
Messina S, Mariano R, Geraldes R, et al. The influence of smoking on the pattern of disability and relapse risk in AQP4-positive Neuromyelitis Optica Spectrum Disorder, MOG-Ab Disease and Multiple Sclerosis. Mult. Scler. Relat. Disord.,2021, 49: 102773. DOI: 10.1016/j.msard.2021.102773
[6]
Lavery A M, Collins B N, Waldman A T, et al. The contribution of secondhand tobacco smoke exposure to pediatric multiple sclerosis risk. Mult. Scler.,2019, 25 (4): 515–522. DOI: 10.1177/1352458518757089
[7]
Pittas F, Ponsonby A L, van der Mei I A F, et al. Smoking is associated with progressive disease course and increased progression in clinical disability in a prospective cohort of people with multiple sclerosis. J. Neurol.,2009, 256 (4): 577–585. DOI: 10.1007/s00415-009-0120-2
[8]
Petersen E R, Oturai A B, Koch-Henriksen N, et al. Smoking affects the interferon beta treatment response in multiple sclerosis. Neurology,2018, 90 (7): e593–e600. DOI: 10.1212/WNL.0000000000004949
[9]
Munger K L, Fitzgerald K C, Freedman M S, et al. No association of multiple sclerosis activity and progression with EBV or tobacco use in BENEFIT. Neurology,2015, 85 (19): 1694–1701. DOI: 10.1212/WNL.0000000000002099
[10]
Weiland T J, Hadgkiss E J, Jelinek G A, et al. The association of alcohol consumption and smoking with quality of life, disability and disease activity in an international sample of people with multiple sclerosis. J. Neurol. Sci.,2014, 336: 211–219. DOI: 10.1016/j.jns.2013.10.046
[11]
Kvistad S, Myhr K M, Holmøy T, et al. No association of tobacco use and disease activity in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm.,2016, 3 (4): e260. DOI: 10.1212/NXI.0000000000000260
[12]
Briggs F B S, Yu J C, Davis M F, et al. Multiple sclerosis risk factors contribute to onset heterogeneity. Mult. Scler. Relat. Disord.,2019, 28: 11–16. DOI: 10.1016/j.msard.2018.12.007
[13]
Petersen E R, Søndergaard H B, Laursen J H, et al. Smoking is associated with increased disease activity during natalizumab treatment in multiple sclerosis. Mult. Scler.,2019, 25 (9): 1298–1305. DOI: 10.1177/1352458518791753
[14]
Polman C H, Reingold S C, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol.,2011, 69 (2): 292–302. DOI: 10.1002/ana.22366
[15]
Thompson A J, Banwell B L, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol.,2018, 17 (2): 162–173. DOI: 10.1016/S1474-4422(17)30470-2
[16]
Wingerchuk D M, Banwell B, Bennett J L, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology,2015, 85 (2): 177–189. DOI: 10.1212/WNL.0000000000001729
[17]
Hedström A K, Olsson T, Alfredsson L. Smoking is a major preventable risk factor for multiple sclerosis. Mult. Scler.,2016, 22 (8): 1021–1026. DOI: 10.1177/1352458515609794
[18]
Kurtzke J F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology,1983, 33 (11): 1444–1452. DOI: 10.1212/WNL.33.11.1444
[19]
Roxburgh R H S R, Seaman S R, Masterman T, et al. Multiple Sclerosis Severity Score: Using disability and disease duration to rate disease severity. Neurology,2005, 64 (7): 1144–1151. DOI: 10.1212/01.WNL.0000156155.19270.F8
[20]
Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology,2015, 44 (4): 199–214. DOI: 10.1159/000382130
[21]
Tettey P, Simpson S Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult. Scler.,2014, 20 (13): 1737–1744. DOI: 10.1177/1352458514533162
[22]
Manouchehrinia A, Tench C R, Maxted J, et al. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain,2013, 136: 2298–2304. DOI: 10.1093/brain/awt139
[23]
Ivashynka A, Copetti M, Naldi P, et al. The impact of lifetime alcohol and cigarette smoking loads on multiple sclerosis severity. Front. Neurol.,2019, 10: 866. DOI: 10.3389/fneur.2019.00866
[24]
Paz-Ballesteros W C, Monterrubio-Flores E A, de Jesús Flores-Rivera J, et al. Cigarette smoking, alcohol consumption and overweight in multiple sclerosis: disability progression. Arch. Med. Res.,2017, 48 (1): 113–120. DOI: 10.1016/j.arcmed.2017.03.002
[25]
D'hooghe M B, Haentjens P, Nagels G, et al. Alcohol, coffee, fish, smoking and disease progression in multiple sclerosis. Eur. J. Neurol.,2012, 19 (4): 616–624. DOI: 10.1111/j.1468-1331.2011.03596.x
[26]
Kinga M, Balasa R. Effect of serum 25(OH) D level, cigarette smoking and oral contraceptive use on clinical course of relapsing-remitting multiple sclerosis in a group of female patients. Romanian Journal of Neurology,2015, 14 (4): 214–218. DOI: 10.37897/RJN.2015.4.5
[27]
Al Wutayd O, Mohamed A G, Saeedi J, et al. Environmental exposures and the risk of multiple sclerosis in Saudi Arabia. BMC Neurol.,2018, 18 (1): 86. DOI: 10.1186/s12883-018-1090-8
[28]
Tao C, Simpson S Jr, Taylor B V, et al. Onset symptoms, tobacco smoking, and progressive-onset phenotype are associated with a delayed onset of multiple sclerosis, and marijuana use with an earlier onset. Front. Neurol.,2018, 9: 418. DOI: 10.3389/fneur.2018.00418
[29]
McDowell T Y, Amr S, Culpepper W J, et al. Sun exposure, vitamin D and age at disease onset in relapsing multiple sclerosis. Neuroepidemiology,2011, 36 (1): 39–45. DOI: 10.1159/000322512
[30]
Hedström A K, Hillert J, Olsson T, et al. Smoking and multiple sclerosis susceptibility. Eur. J. Epidemiol.,2013, 28 (11): 867–874. DOI: 10.1007/s10654-013-9853-4
[31]
Hedstrom A K, Baarnhielm M, Olsson T, et al. Tobacco smoking, but not Swedish snuff use, increases the risk of multiple sclerosis. Neurology,2009, 73 (9): 696–701. DOI: 10.1212/WNL.0b013e3181b59c40
[32]
Alrouji M, Manouchehrinia A, Gran B, et al. Effects of cigarette smoke on immunity, neuroinflammation and multiple sclerosis. J. Neuroimmunol.,2019, 329: 24–34. DOI: 10.1016/j.jneuroim.2018.10.004
[33]
Jin H J, Li H T, Sui H X, et al. Nicotine stimulated bone marrow-derived dendritic cells could augment HBV specific CTL priming by activating PI3K-Akt pathway. Immunol. Lett.,2012, 146: 40–49. DOI: 10.1016/j.imlet.2012.02.015
[34]
Gao Z, Nissen J C, Ji K, et al. The experimental autoimmune encephalomyelitis disease course is modulated by nicotine and other cigarette smoke components. PLoS One,2014, 9 (9): e107979. DOI: 10.1371/journal.pone.0107979
[35]
de Jonge W J, Ulloa L. The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br. J. Pharmacol.,2007, 151 (7): 915–929. DOI: 10.1038/sj.bjp.0707264
[36]
Tracey K J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Invest.,2007, 117 (2): 289–296. DOI: 10.1172/JCI30555
[37]
Filippini P, Cesario A, Fini M, et al. The Yin and Yang of non-neuronal α7-nicotinic receptors in inflammation and autoimmunity. Curr. Drug Targets,2012, 13 (5): 644–655. DOI: 10.2174/138945012800399008






 DownLoad:
DownLoad: