
| [1] |
Höftberger R, Lassmann H. Inflammatory demyelinating diseases of the central nervous system. Handb. Clin. Neurol., 2017, 145: 263–283. doi: 10.1016/B978-0-12-802395-2.00019-5
|
| [2] |
Lennon V A, Wingerchuk D M, Kryzer T J, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet, 2004, 364 (9451): 2106–2112. doi: 10.1016/S0140-6736(04)17551-X
|
| [3] |
Tian D C, Zhang C Y, Yuan M, et al. Incidence of multiple sclerosis in China: A nationwide hospital-based study. Lancet Reg. Health West. Pac., 2020, 1: 100010. doi: 10.1016/j.lanwpc.2020.100010
|
| [4] |
Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: A review. JAMA Neurol., 2020, 77 (2): 245–253. doi: 10.1001/jamaneurol.2019.4271
|
| [5] |
Messina S, Mariano R, Geraldes R, et al. The influence of smoking on the pattern of disability and relapse risk in AQP4-positive Neuromyelitis Optica Spectrum Disorder, MOG-Ab Disease and Multiple Sclerosis. Mult. Scler. Relat. Disord., 2021, 49: 102773. doi: 10.1016/j.msard.2021.102773
|
| [6] |
Lavery A M, Collins B N, Waldman A T, et al. The contribution of secondhand tobacco smoke exposure to pediatric multiple sclerosis risk. Mult. Scler., 2019, 25 (4): 515–522. doi: 10.1177/1352458518757089
|
| [7] |
Pittas F, Ponsonby A L, van der Mei I A F, et al. Smoking is associated with progressive disease course and increased progression in clinical disability in a prospective cohort of people with multiple sclerosis. J. Neurol., 2009, 256 (4): 577–585. doi: 10.1007/s00415-009-0120-2
|
| [8] |
Petersen E R, Oturai A B, Koch-Henriksen N, et al. Smoking affects the interferon beta treatment response in multiple sclerosis. Neurology, 2018, 90 (7): e593–e600. doi: 10.1212/WNL.0000000000004949
|
| [9] |
Munger K L, Fitzgerald K C, Freedman M S, et al. No association of multiple sclerosis activity and progression with EBV or tobacco use in BENEFIT. Neurology, 2015, 85 (19): 1694–1701. doi: 10.1212/WNL.0000000000002099
|
| [10] |
Weiland T J, Hadgkiss E J, Jelinek G A, et al. The association of alcohol consumption and smoking with quality of life, disability and disease activity in an international sample of people with multiple sclerosis. J. Neurol. Sci., 2014, 336: 211–219. doi: 10.1016/j.jns.2013.10.046
|
| [11] |
Kvistad S, Myhr K M, Holmøy T, et al. No association of tobacco use and disease activity in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm., 2016, 3 (4): e260. doi: 10.1212/NXI.0000000000000260
|
| [12] |
Briggs F B S, Yu J C, Davis M F, et al. Multiple sclerosis risk factors contribute to onset heterogeneity. Mult. Scler. Relat. Disord., 2019, 28: 11–16. doi: 10.1016/j.msard.2018.12.007
|
| [13] |
Petersen E R, Søndergaard H B, Laursen J H, et al. Smoking is associated with increased disease activity during natalizumab treatment in multiple sclerosis. Mult. Scler., 2019, 25 (9): 1298–1305. doi: 10.1177/1352458518791753
|
| [14] |
Polman C H, Reingold S C, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol., 2011, 69 (2): 292–302. doi: 10.1002/ana.22366
|
| [15] |
Thompson A J, Banwell B L, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol., 2018, 17 (2): 162–173. doi: 10.1016/S1474-4422(17)30470-2
|
| [16] |
Wingerchuk D M, Banwell B, Bennett J L, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology, 2015, 85 (2): 177–189. doi: 10.1212/WNL.0000000000001729
|
| [17] |
Hedström A K, Olsson T, Alfredsson L. Smoking is a major preventable risk factor for multiple sclerosis. Mult. Scler., 2016, 22 (8): 1021–1026. doi: 10.1177/1352458515609794
|
| [18] |
Kurtzke J F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology, 1983, 33 (11): 1444–1452. doi: 10.1212/WNL.33.11.1444
|
| [19] |
Roxburgh R H S R, Seaman S R, Masterman T, et al. Multiple Sclerosis Severity Score: Using disability and disease duration to rate disease severity. Neurology, 2005, 64 (7): 1144–1151. doi: 10.1212/01.WNL.0000156155.19270.F8
|
| [20] |
Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology, 2015, 44 (4): 199–214. doi: 10.1159/000382130
|
| [21] |
Tettey P, Simpson S Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult. Scler., 2014, 20 (13): 1737–1744. doi: 10.1177/1352458514533162
|
| [22] |
Manouchehrinia A, Tench C R, Maxted J, et al. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain, 2013, 136: 2298–2304. doi: 10.1093/brain/awt139
|
| [23] |
Ivashynka A, Copetti M, Naldi P, et al. The impact of lifetime alcohol and cigarette smoking loads on multiple sclerosis severity. Front. Neurol., 2019, 10: 866. doi: 10.3389/fneur.2019.00866
|
| [24] |
Paz-Ballesteros W C, Monterrubio-Flores E A, de Jesús Flores-Rivera J, et al. Cigarette smoking, alcohol consumption and overweight in multiple sclerosis: disability progression. Arch. Med. Res., 2017, 48 (1): 113–120. doi: 10.1016/j.arcmed.2017.03.002
|
| [25] |
D'hooghe M B, Haentjens P, Nagels G, et al. Alcohol, coffee, fish, smoking and disease progression in multiple sclerosis. Eur. J. Neurol., 2012, 19 (4): 616–624. doi: 10.1111/j.1468-1331.2011.03596.x
|
| [26] |
Kinga M, Balasa R. Effect of serum 25(OH) D level, cigarette smoking and oral contraceptive use on clinical course of relapsing-remitting multiple sclerosis in a group of female patients. Romanian Journal of Neurology, 2015, 14 (4): 214–218. doi: 10.37897/RJN.2015.4.5
|
| [27] |
Al Wutayd O, Mohamed A G, Saeedi J, et al. Environmental exposures and the risk of multiple sclerosis in Saudi Arabia. BMC Neurol., 2018, 18 (1): 86. doi: 10.1186/s12883-018-1090-8
|
| [28] |
Tao C, Simpson S Jr, Taylor B V, et al. Onset symptoms, tobacco smoking, and progressive-onset phenotype are associated with a delayed onset of multiple sclerosis, and marijuana use with an earlier onset. Front. Neurol., 2018, 9: 418. doi: 10.3389/fneur.2018.00418
|
| [29] |
McDowell T Y, Amr S, Culpepper W J, et al. Sun exposure, vitamin D and age at disease onset in relapsing multiple sclerosis. Neuroepidemiology, 2011, 36 (1): 39–45. doi: 10.1159/000322512
|
| [30] |
Hedström A K, Hillert J, Olsson T, et al. Smoking and multiple sclerosis susceptibility. Eur. J. Epidemiol., 2013, 28 (11): 867–874. doi: 10.1007/s10654-013-9853-4
|
| [31] |
Hedstrom A K, Baarnhielm M, Olsson T, et al. Tobacco smoking, but not Swedish snuff use, increases the risk of multiple sclerosis. Neurology, 2009, 73 (9): 696–701. doi: 10.1212/WNL.0b013e3181b59c40
|
| [32] |
Alrouji M, Manouchehrinia A, Gran B, et al. Effects of cigarette smoke on immunity, neuroinflammation and multiple sclerosis. J. Neuroimmunol., 2019, 329: 24–34. doi: 10.1016/j.jneuroim.2018.10.004
|
| [33] |
Jin H J, Li H T, Sui H X, et al. Nicotine stimulated bone marrow-derived dendritic cells could augment HBV specific CTL priming by activating PI3K-Akt pathway. Immunol. Lett., 2012, 146: 40–49. doi: 10.1016/j.imlet.2012.02.015
|
| [34] |
Gao Z, Nissen J C, Ji K, et al. The experimental autoimmune encephalomyelitis disease course is modulated by nicotine and other cigarette smoke components. PLoS One, 2014, 9 (9): e107979. doi: 10.1371/journal.pone.0107979
|
| [35] |
de Jonge W J, Ulloa L. The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br. J. Pharmacol., 2007, 151 (7): 915–929. doi: 10.1038/sj.bjp.0707264
|
| [36] |
Tracey K J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Invest., 2007, 117 (2): 289–296. doi: 10.1172/JCI30555
|
| [37] |
Filippini P, Cesario A, Fini M, et al. The Yin and Yang of non-neuronal α7-nicotinic receptors in inflammation and autoimmunity. Curr. Drug Targets, 2012, 13 (5): 644–655. doi: 10.2174/138945012800399008
|
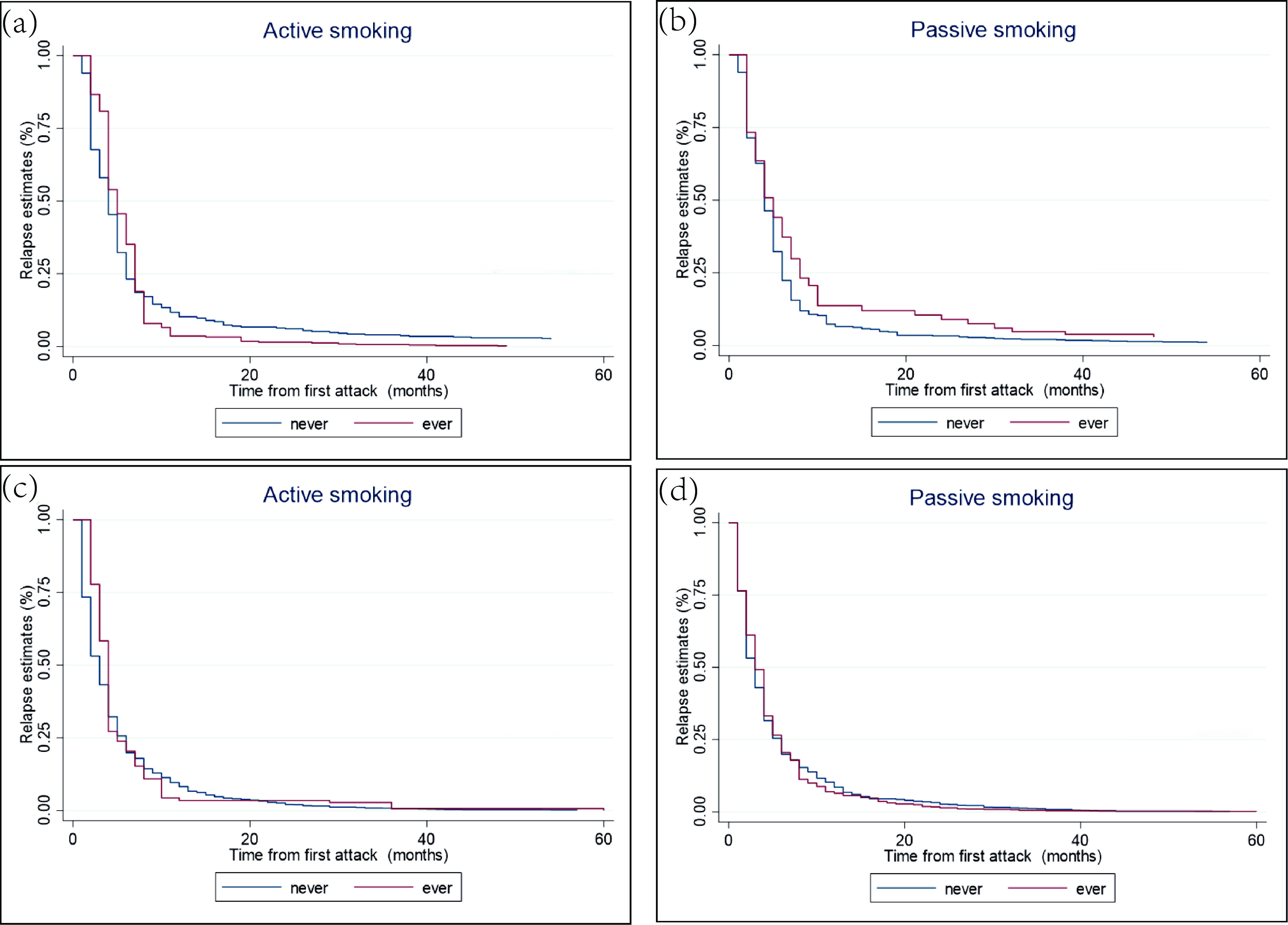
Figure 1. Kaplan‒Meier analysis of (a, b) time to relapse in the MS cohort and (c, d) time to relapse in the NMOSD cohort.
| [1] |
Höftberger R, Lassmann H. Inflammatory demyelinating diseases of the central nervous system. Handb. Clin. Neurol., 2017, 145: 263–283. doi: 10.1016/B978-0-12-802395-2.00019-5
|
| [2] |
Lennon V A, Wingerchuk D M, Kryzer T J, et al. A serum autoantibody marker of neuromyelitis optica: distinction from multiple sclerosis. Lancet, 2004, 364 (9451): 2106–2112. doi: 10.1016/S0140-6736(04)17551-X
|
| [3] |
Tian D C, Zhang C Y, Yuan M, et al. Incidence of multiple sclerosis in China: A nationwide hospital-based study. Lancet Reg. Health West. Pac., 2020, 1: 100010. doi: 10.1016/j.lanwpc.2020.100010
|
| [4] |
Rosso M, Chitnis T. Association between cigarette smoking and multiple sclerosis: A review. JAMA Neurol., 2020, 77 (2): 245–253. doi: 10.1001/jamaneurol.2019.4271
|
| [5] |
Messina S, Mariano R, Geraldes R, et al. The influence of smoking on the pattern of disability and relapse risk in AQP4-positive Neuromyelitis Optica Spectrum Disorder, MOG-Ab Disease and Multiple Sclerosis. Mult. Scler. Relat. Disord., 2021, 49: 102773. doi: 10.1016/j.msard.2021.102773
|
| [6] |
Lavery A M, Collins B N, Waldman A T, et al. The contribution of secondhand tobacco smoke exposure to pediatric multiple sclerosis risk. Mult. Scler., 2019, 25 (4): 515–522. doi: 10.1177/1352458518757089
|
| [7] |
Pittas F, Ponsonby A L, van der Mei I A F, et al. Smoking is associated with progressive disease course and increased progression in clinical disability in a prospective cohort of people with multiple sclerosis. J. Neurol., 2009, 256 (4): 577–585. doi: 10.1007/s00415-009-0120-2
|
| [8] |
Petersen E R, Oturai A B, Koch-Henriksen N, et al. Smoking affects the interferon beta treatment response in multiple sclerosis. Neurology, 2018, 90 (7): e593–e600. doi: 10.1212/WNL.0000000000004949
|
| [9] |
Munger K L, Fitzgerald K C, Freedman M S, et al. No association of multiple sclerosis activity and progression with EBV or tobacco use in BENEFIT. Neurology, 2015, 85 (19): 1694–1701. doi: 10.1212/WNL.0000000000002099
|
| [10] |
Weiland T J, Hadgkiss E J, Jelinek G A, et al. The association of alcohol consumption and smoking with quality of life, disability and disease activity in an international sample of people with multiple sclerosis. J. Neurol. Sci., 2014, 336: 211–219. doi: 10.1016/j.jns.2013.10.046
|
| [11] |
Kvistad S, Myhr K M, Holmøy T, et al. No association of tobacco use and disease activity in multiple sclerosis. Neurol. Neuroimmunol. Neuroinflamm., 2016, 3 (4): e260. doi: 10.1212/NXI.0000000000000260
|
| [12] |
Briggs F B S, Yu J C, Davis M F, et al. Multiple sclerosis risk factors contribute to onset heterogeneity. Mult. Scler. Relat. Disord., 2019, 28: 11–16. doi: 10.1016/j.msard.2018.12.007
|
| [13] |
Petersen E R, Søndergaard H B, Laursen J H, et al. Smoking is associated with increased disease activity during natalizumab treatment in multiple sclerosis. Mult. Scler., 2019, 25 (9): 1298–1305. doi: 10.1177/1352458518791753
|
| [14] |
Polman C H, Reingold S C, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol., 2011, 69 (2): 292–302. doi: 10.1002/ana.22366
|
| [15] |
Thompson A J, Banwell B L, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol., 2018, 17 (2): 162–173. doi: 10.1016/S1474-4422(17)30470-2
|
| [16] |
Wingerchuk D M, Banwell B, Bennett J L, et al. International consensus diagnostic criteria for neuromyelitis optica spectrum disorders. Neurology, 2015, 85 (2): 177–189. doi: 10.1212/WNL.0000000000001729
|
| [17] |
Hedström A K, Olsson T, Alfredsson L. Smoking is a major preventable risk factor for multiple sclerosis. Mult. Scler., 2016, 22 (8): 1021–1026. doi: 10.1177/1352458515609794
|
| [18] |
Kurtzke J F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology, 1983, 33 (11): 1444–1452. doi: 10.1212/WNL.33.11.1444
|
| [19] |
Roxburgh R H S R, Seaman S R, Masterman T, et al. Multiple Sclerosis Severity Score: Using disability and disease duration to rate disease severity. Neurology, 2005, 64 (7): 1144–1151. doi: 10.1212/01.WNL.0000156155.19270.F8
|
| [20] |
Kalincik T. Multiple sclerosis relapses: epidemiology, outcomes and management. A systematic review. Neuroepidemiology, 2015, 44 (4): 199–214. doi: 10.1159/000382130
|
| [21] |
Tettey P, Simpson S Jr, Taylor B, et al. An adverse lipid profile is associated with disability and progression in disability, in people with MS. Mult. Scler., 2014, 20 (13): 1737–1744. doi: 10.1177/1352458514533162
|
| [22] |
Manouchehrinia A, Tench C R, Maxted J, et al. Tobacco smoking and disability progression in multiple sclerosis: United Kingdom cohort study. Brain, 2013, 136: 2298–2304. doi: 10.1093/brain/awt139
|
| [23] |
Ivashynka A, Copetti M, Naldi P, et al. The impact of lifetime alcohol and cigarette smoking loads on multiple sclerosis severity. Front. Neurol., 2019, 10: 866. doi: 10.3389/fneur.2019.00866
|
| [24] |
Paz-Ballesteros W C, Monterrubio-Flores E A, de Jesús Flores-Rivera J, et al. Cigarette smoking, alcohol consumption and overweight in multiple sclerosis: disability progression. Arch. Med. Res., 2017, 48 (1): 113–120. doi: 10.1016/j.arcmed.2017.03.002
|
| [25] |
D'hooghe M B, Haentjens P, Nagels G, et al. Alcohol, coffee, fish, smoking and disease progression in multiple sclerosis. Eur. J. Neurol., 2012, 19 (4): 616–624. doi: 10.1111/j.1468-1331.2011.03596.x
|
| [26] |
Kinga M, Balasa R. Effect of serum 25(OH) D level, cigarette smoking and oral contraceptive use on clinical course of relapsing-remitting multiple sclerosis in a group of female patients. Romanian Journal of Neurology, 2015, 14 (4): 214–218. doi: 10.37897/RJN.2015.4.5
|
| [27] |
Al Wutayd O, Mohamed A G, Saeedi J, et al. Environmental exposures and the risk of multiple sclerosis in Saudi Arabia. BMC Neurol., 2018, 18 (1): 86. doi: 10.1186/s12883-018-1090-8
|
| [28] |
Tao C, Simpson S Jr, Taylor B V, et al. Onset symptoms, tobacco smoking, and progressive-onset phenotype are associated with a delayed onset of multiple sclerosis, and marijuana use with an earlier onset. Front. Neurol., 2018, 9: 418. doi: 10.3389/fneur.2018.00418
|
| [29] |
McDowell T Y, Amr S, Culpepper W J, et al. Sun exposure, vitamin D and age at disease onset in relapsing multiple sclerosis. Neuroepidemiology, 2011, 36 (1): 39–45. doi: 10.1159/000322512
|
| [30] |
Hedström A K, Hillert J, Olsson T, et al. Smoking and multiple sclerosis susceptibility. Eur. J. Epidemiol., 2013, 28 (11): 867–874. doi: 10.1007/s10654-013-9853-4
|
| [31] |
Hedstrom A K, Baarnhielm M, Olsson T, et al. Tobacco smoking, but not Swedish snuff use, increases the risk of multiple sclerosis. Neurology, 2009, 73 (9): 696–701. doi: 10.1212/WNL.0b013e3181b59c40
|
| [32] |
Alrouji M, Manouchehrinia A, Gran B, et al. Effects of cigarette smoke on immunity, neuroinflammation and multiple sclerosis. J. Neuroimmunol., 2019, 329: 24–34. doi: 10.1016/j.jneuroim.2018.10.004
|
| [33] |
Jin H J, Li H T, Sui H X, et al. Nicotine stimulated bone marrow-derived dendritic cells could augment HBV specific CTL priming by activating PI3K-Akt pathway. Immunol. Lett., 2012, 146: 40–49. doi: 10.1016/j.imlet.2012.02.015
|
| [34] |
Gao Z, Nissen J C, Ji K, et al. The experimental autoimmune encephalomyelitis disease course is modulated by nicotine and other cigarette smoke components. PLoS One, 2014, 9 (9): e107979. doi: 10.1371/journal.pone.0107979
|
| [35] |
de Jonge W J, Ulloa L. The alpha7 nicotinic acetylcholine receptor as a pharmacological target for inflammation. Br. J. Pharmacol., 2007, 151 (7): 915–929. doi: 10.1038/sj.bjp.0707264
|
| [36] |
Tracey K J. Physiology and immunology of the cholinergic antiinflammatory pathway. J. Clin. Invest., 2007, 117 (2): 289–296. doi: 10.1172/JCI30555
|
| [37] |
Filippini P, Cesario A, Fini M, et al. The Yin and Yang of non-neuronal α7-nicotinic receptors in inflammation and autoimmunity. Curr. Drug Targets, 2012, 13 (5): 644–655. doi: 10.2174/138945012800399008
|

ISSN 0253-2778
CN 34-1054/N
Copyright © Editorial Office of JUSTC, All Rights Reserved. 皖ICP备05002528号
Supported by:
Beijing Renhe Information Technology Co. Ltd





 DownLoad:
DownLoad: